


Grey Zones in Breast Cytology
The application of fine needle aspiration cytology in the diagnosis of palpable breast lesions was first introduced by Martin and Ellis in 1930 and since then it has been entrenched as an important tool. FNAC of the breast is a simple, cost-effective, less traumatic, sensitive and a rapid diagnostic method. It continues to play an integral part in the management of breast lesions.
Correlation of FNAC results with clinical and imaging studies is referred to as the Triple test and many studies have revealed 100 % diagnostic accuracy.
According to the National Cancer Institute (NCI) guidelines in 1996 and NHSBSP guidelines (1992), FNAC of the breasts were categorized into five categories. Categories such as C1, C2 and C5 are usually straightforward and do not generally pose difficulties. However, interpretation of C3 and C4 categories are challenging and there exists significant inter-observer variation as no strict criteria are present for the diagnosis of these categories.

A lesion termed as “atypia probably benign” (C3) means that it has predominantly benign cytomorphology with the presence of nuclear pleomorphism or cellular discohesion. In addition, an increase in cellularity can also be associated with any of these features. The lesions termed as “suspicious of malignancy” (C4) include those with some cells showing features of malignancy, in a material that is not diagnostic due to its scantiness, poor preservation, or poor preparation.
Importance of these two categories (C3 & C4) lies in the buffering they provide to both the cytopathologists and clinicians. It implies the limitation and diagnostic difficulty on the part of the pathologist in accurately classifying some of the lesions regardless of adequate sampling where as it guides the clinician to follow-up such patients with a repeat FNAC or core needle biopsy.
False Negatives |
False Positives |
l The major causes of difference on cytology and histopathology include- – Technical: Low cellularity. – Low Grade Malignancies: Ductal carcinoma insitu and Grade I Invasive ductal carcinoma, Lobular carcinoma insitu and Benign Phyllodes.
l Atypical epithelial hyperplasia and Low grade carcinoma Insitu are similar entities, – Quantitatively different (the former being smaller). – Qualitatively the same (in terms of cellular details) |
l The cytologic diagnosis of Papillary lesions is problematic because till date there are no well-defined cytological criteria to differentiate between benign and malignant papillary lesions. l Other common lesions giving a false positive diagnosis for malignancy include Ductal and Lobular hyperplasia.
|
EPITHELIAL HYPERPLASIA
|
ATYPICAL DUCTAL HYPERPLASIA |
LOW GRADE DUCTAL CARCINOMA INSITU |
Cohesive epithelial cell clusters as well as single cells |
Large sheets of cohesive cells |
Large and small sheets of cohesive cells. |
Streaming pattern, nuclear atypia |
Holes suggesting cribriforming |
Same as ADH plus papillary clusters, mild nuclear atypia |
Focal crowding and overlapping of nuclei, myoepithelial cells. |
Focal crowding, overlapping of nuclei, holes, mild to moderate atypia |
Naked bipolar cells absent, absent myoepithelial cells. |
Few calcium granules |
Occasional deposit |
Necrotic debris |
Stratification of C3 and C4 cases is beneficial as it identifies groups of patients who are more likely to have either benign or malignant outcomes. Whereas clubbing of C3 and C4 categories termed as equivocal category is also suggested in many studies as it is believed that trucut biopsy should be done for this combined category as the incidence of malignancy is significant in both the subgroups.
CASES CAUSING DIAGNOSTIC DILEMMA ENCOUNTERED IN OUR LAB:
One of our cases that were reported as a C3 lesion on FNAC turned out to be Invasive ductal carcinoma on trucut biopsy.
C3 on FNAC-

Invasive Ductal Carcinoma on Trucut Biopsy–

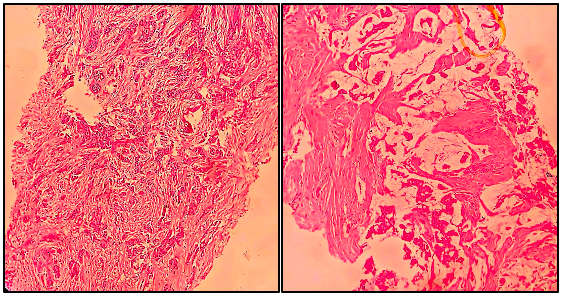
Other case was of a middle aged female with a huge breast lump occupying whole of the breast. On ultrasonography, it was diagnosed as a Birads IVb lesion and on cytology, a diagnosis of Benign proliferative breast disease; possibly Giant fibroadenoma with cystic change (Category C2) was rendered. Following this, lumpectomy was done and on histopathological examination it turned out to be Benign Phyllodes tumor.
On FNAC– Giant Fibroadenoma with Cystic change (Category C2)-

Lumpectomy specimen– Benign Phyllodes Tumor
